.png)

Clothing as Medical Infrastructure
- The TechStyles Team
- Mar 11
- 5 min read
Updated: Apr 8

Wearable health began as an extension of the clinic.
We moved monitoring from hospital rooms to wrists. From episodic measurements to continuous streams. From clipboard surveys to dashboards.
That shift mattered. But it was only the first step.
Now the question facing biopharma and med-tech innovation teams is more consequential:
Not just what can we measure but where does meaningful data actually live?
Because the reality is this: Most clinically relevant behavior does not happen in a lab.
It happens in kitchens. On stairs. In parking lots. At work. During recovery. In moments of fatigue. In private frustration. In small adaptations no protocol ever captured.
If wearable health is meant to inform real-world evidence, decentralized trials, and long-term outcomes, then we need to rethink the interface between the body and data.
Clothing may be that interface.
Not as fashion.
Not as novelty.
But as medical infrastructure.
The Limits of Lab-Only Data
Clinical environments are optimized for control.
Controlled temperature. Controlled movement. Controlled instruction. Controlled observation.
That control is necessary for safety and validation. But it introduces a structural constraint:
It filters out context.
And context is where adherence, mobility, fatigue, compensation patterns, and daily burden actually show up.
A wearable that performs perfectly in a clinic may fail quietly the moment it enters daily life.
Not because the sensors are flawed. But because the environment changes.
Real-world evidence depends on real-world use.
And real-world use depends on human fit.
Clothing Is Already Infrastructure
We rarely think of clothing as infrastructure. But it is.
Clothing:
Stays in contact with the body for extended durations
Moves with joints and muscles
Adapts to posture and activity
Integrates into identity and routine
Crosses settings without friction
Unlike many external devices, clothing is not an “add-on.” It is the baseline.
That baseline status is precisely why it matters for regulated health innovation.
If data capture can be integrated into what people already wear, without stigma, without burden, without interruption, adherence shifts from conscious compliance to natural behavior.
This is not cosmetic design. This is a deployment strategy.
Non-Lab Data Is Not Optional
For biopharma teams exploring digital endpoints, remote monitoring, or decentralized trials, non-lab data is not a secondary signal. It is increasingly the primary one.
Regulators are signaling openness to digital measures. Payers are demanding real-world performance. Clinical teams are under pressure to demonstrate longitudinal value.
But evidence built on partial adoption collapses under scrutiny because data streams break when wearables are abandoned.
Endpoints weaken when devices are used inconsistently.
Compliance degrades when tools disrupt identity or daily function.
This is not a behavioral flaw. It is a design constraint that was not resolved early enough.
Clothing as infrastructure addresses this constraint directly.
Beyond Vitals: Functional and Behavioral Signals
The first generation of wearables prioritized vitals.Heart rate. Steps. Sleep. Blood pressure.
Important metrics but hardly comprehensive.
For many therapeutic areas, the most meaningful indicators are functional and behavioral:
Gait stability
Fatigue patterns
Fine motor control
Strength variability
Posture adaptation
Frequency of task completion
Balance events
Activity clustering
Adherence to therapy routines
These signals live in movement, pressure, micro-adjustment, and repetition.
They do not always live on the wrist.
Clothing, when properly designed, has access to these domains naturally.
Embedded sensors in garments, compression systems, adaptive fabrics, and textile-based interfaces can capture data that reflects how a person actually lives with a condition.
That data may feel messy and uncontrolled but it is harder to fake. Harder to misinterpret. Harder to isolate from context.
Because it is contextual by design.
The Human Factor Is the Stability Layer
There is a misconception in innovation circles that infrastructure means hardware. But in regulated wearable systems, infrastructure means stability.
Stability of use.
Stability of signal.
Stability of adoption.
Clothing succeeds as infrastructure when it becomes invisible and when it does not require constant cognitive effort to engage.
A wearable that must be remembered, charged, adjusted, explained, and tolerated is fragile.
A wearable that integrates into daily clothing patterns is resilient.
This distinction becomes critical in:
Decentralized clinical trials
Long-term chronic condition monitoring
Real-world evidence generation
Post-market surveillance
Home-based rehabilitation
When patients are responsible for self-managed use, resilience determines evidence quality.
And resilience is a human design outcome.
Identity and Dignity as Clinical Variables
In regulated environments, we often reduce design variables to comfort and usability.
But identity and dignity are equally powerful.
If a wearable signals illness too loudly, patients may disengage.
If a device feels stigmatizing, it may be worn inconsistently.
If clothing-based systems respect self-expression and normalcy, persistence increases.
This is not philosophy. It is adherence science.
Patients are not passive participants in data collection. They are decision-makers navigating their own experience.
When clothing aligns with identity rather than undermining it, it stabilizes adoption and stable adoption produces reliable evidence.
Pre-Scale Is Where Infrastructure Is Decided
By the time a wearable platform reaches manufacturing scale, most structural decisions are locked.
Sensor placement. Form factor. Interface logic. Material choices. Onboarding complexity.
If clothing integration is not considered early, retrofitting becomes expensive — and often incomplete.
This is why infrastructure thinking belongs in the pre-scale phase:
Problem Analysis → Prototype → Pilot → Real-World Use → Scale Handoff
In early prototyping cycles, teams can:
Test garments in real environments
Validate comfort over extended durations
Measure adherence patterns
Identify friction before regulatory lock-in
Align digital integration with natural wear cycles
Waiting until scale to address human fit transforms solvable design constraints into systemic risk.
Clothing as Extension of Digital Health Platforms
For digital health strategy teams, clothing does not compete with platforms. It extends them.
Software captures, visualizes, and analyzes. Clothing is the means to capture reality.
When garment-based systems integrate with apps, dashboards, and EHR frameworks, the result is a layered architecture:
Physical layer → data captureDigital layer → interpretationClinical layer → decision support
If the physical layer fails, everything above it destabilizes.
Clothing, properly engineered, strengthens the base.
The Risk Reduction Argument
Biopharma and med-tech innovation teams operate under real constraints:
Regulatory review
Protocol integrity
Endpoint defensibility
Reimbursement alignment
Commercial viability
Wearable systems that do not persist in daily life introduce silent risk.
Low wear time
Inconsistent signal
Protocol deviations
Dropout related to device burden
These are not technical anomalies. They are foreseeable design outcomes.
Integrating sensing into clothing is not a creative flourish. It is a risk mitigation strategy.
When adoption stabilizes, evidence stabilizes.
When evidence stabilizes, regulatory confidence increases.
When regulatory confidence increases, commercial risk decreases.
This is not a linear equation — but the relationship is clear.
From Device Thinking to Infrastructure Thinking
The industry conversation is shifting.
FROM: device features and sensor capabilities
TO: deployment architecture and adoption durability
Clothing belongs in the second category.
It reframes wearables from gadgets to embedded systems.
From optional accessories to integrated infrastructure.
From measurement tools to evidence engines.
Where This Leaves Biopharma and Med-Tech Leaders
The question is no longer whether wearable health matters. It does.
The question is whether the data being generated reflects lived experience with enough fidelity to support regulatory and commercial decisions.
Non-lab data is not a bonus layer. It is the validation layer.
And clothing, when approached as medical infrastructure, offers a pathway to capture that data without increasing patient burden.
This is not about replacing devices.
It is about strengthening the interface between people and systems.
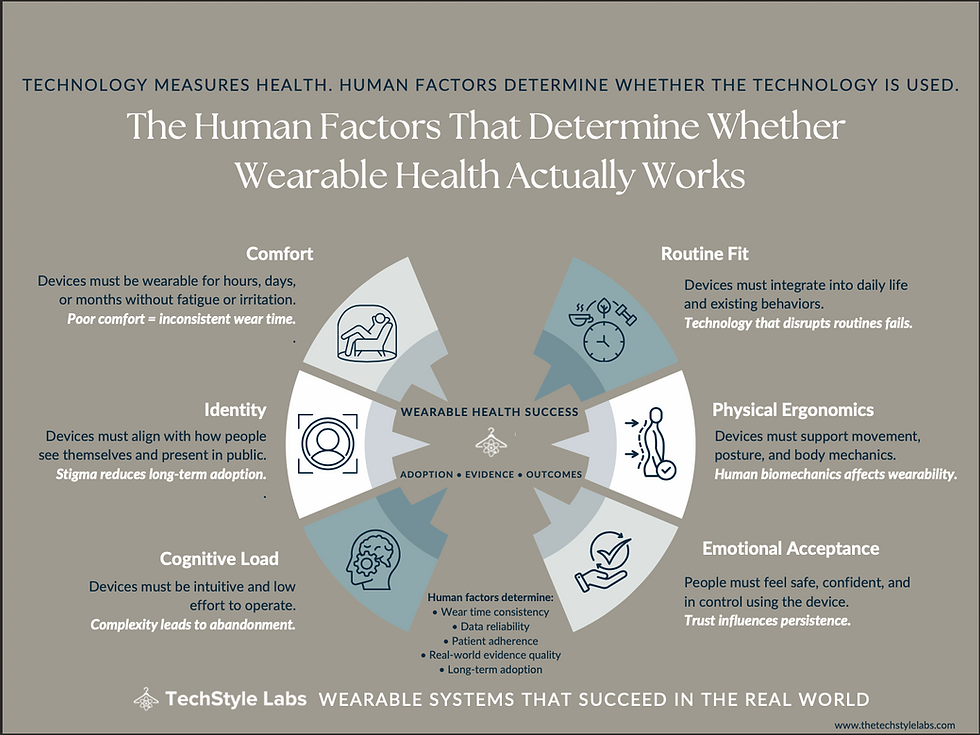
Wearable health needs a human factor.
And sometimes, that human factor looks like the fabric people already trust.
Closing Thought
Technology measures. Infrastructure sustains.
If wearable health is going to support real-world outcomes at scale, we must design systems that people live in, not systems they temporarily tolerate.
For teams exploring wearable innovation in regulated environments, the most important design decisions happen before scale.
That is where infrastructure is set and that is where outcomes are decided.

Comments